The human perirhinal cortex (PRC) plays critical roles in episodic and semantic memory and visual perception. The PRC consists of Brodmann areas 35 and 36 (BA35, BA36). In Alzheimer’s disease (AD), BA35 is the first cortical site affected by neurofibrillary tangle pathology [1], which is closely linked to neural injury in AD. Large anatomical variability, manifested in the form of different cortical folding and branching patterns, makes it difficult to segment the PRC in MRI scans. Pathology studies [2] have found that in ~97% of specimens, the PRC falls into one of three discrete anatomical variants (Figure. 1).
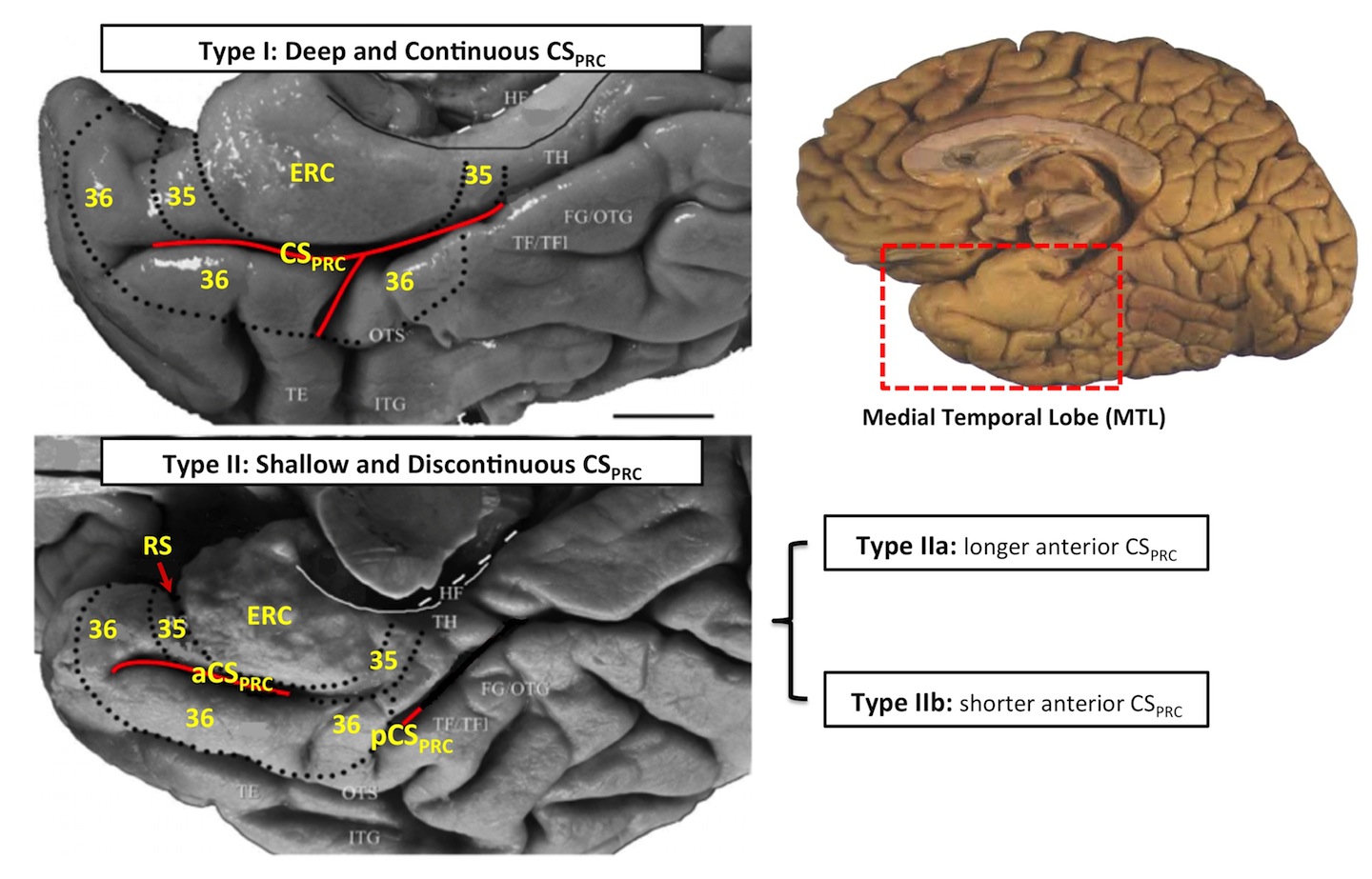
Figure 1. Three anatomical variants of the PRC defined by the folding and branching patterns of the collateral sulcus. Figure adapted from [2]. Abbreviations: ERC = entorhinal cortex; 35, 36 = Brodmann areas 35 and 36; BA35, BA36 = Brodmann areas 35 and 36; PRC = perirhinal cortex; CS = collateral sulcus; CSPRC = the portion of CS adjacent to PRC; aCSPRC/pCSPRC = anterior/posterior CSPRC; HF = hippocampal fissure; RS = rhinal sulcus; FG = fu- siform gyrus; HIPPO = Hippocampus; OTG = occipito-temporal gyrus; OTS = occipito-temporal sulcus; ITG = inferior temporal gyrus; TE, TH, TF = temporal areas TE, TH, TF defined; TFl = lateral subdivisions of area TF.
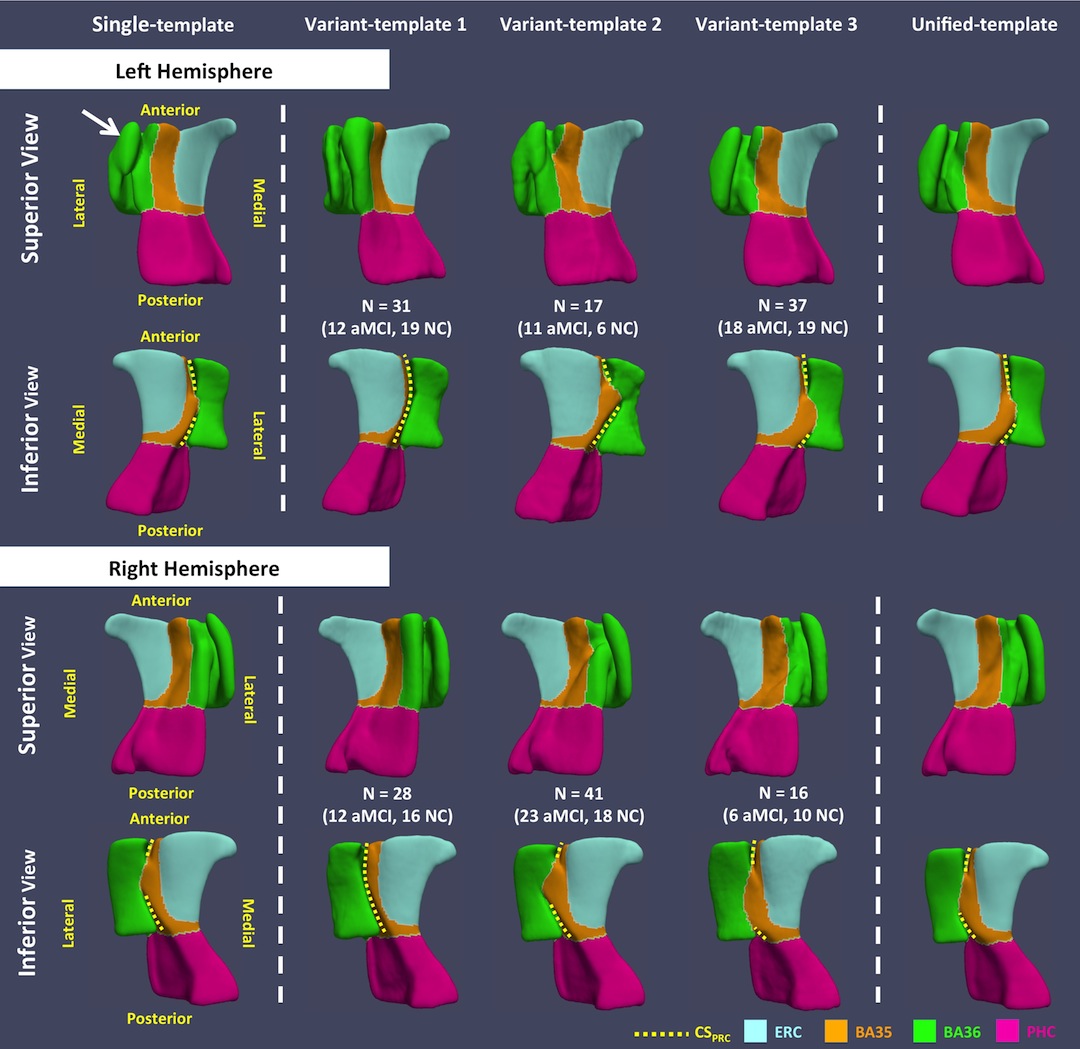
Figure 2. Template meshes obtained using the single-template (ST), variant-template (VT) and unified- template (UT) approaches for both hemispheres. The white arrow points to the structure that connects the medial and lateral borders of BA36 generated by the ST approach, which is anatomically implausible. Yellow dashed curves mark CSPRC in all templates. VT 1 resembles the continuous CSPRC variant. Discontinuous CSPRC is observed in VT 2 and VT 3, and these VTs differ, as expected, by the relative length of the anterior and posterior CSPRC (i.e. anterior CSPRC is shorter in VT 2 while it is longer in VT 3).
Further, when applied to a dataset of patients with amnestic mild cognitive impairment (a-MCI) and normal control, the multi-template approach yielded larger t-statistics in discriminating the two groups compared to the single-template approach, volumetric measurements based on multi-atlas segmentation, and thickness measures extracted from T1w MRI by FreeSurfer [5]. This method may have important utility in the diagnosis and monitoring of early AD, as well as for providing accurate measurements to enhance brain-behavior studies in the medial temporal lobe.
References:
- [1] Braak H, Braak E. Staging of Alzheimer’s disease-related neurofibrillary changes. Neurobiol. Aging 1995; 16: 271–278.
- [2] Ding S-L, Van Hoesen GW. Borders, extent, and topography of human perirhinal cortex as revealed using multiple modern neuroanatomical and pathological markers. Hum. Brain Mapp. 2010; 31: 1359–79.
- [3] Xie L, Pluta JB, Das SR, Wisse LE, Wang H, Mancuso L, Kliot D, Avants BB, Ding SL, Manjón JV, Wolk DA. Multi-Template Analysis of Human Perirhinal Cortex in Brain MRI: Explicitly Accounting for Anatomical Variability. NeuroImage. 2016 Oct 1.
- [4] Yushkevich PA, Pluta JB, Wang H, Xie L, Ding S, Gertje EC, et al. Automated volumetry and regional thickness analysis of hippocampal subfields and medial temporal cortical structures in mild cognitive impairment. Hum. Brain Mapp. 2015; 36: 258–287.
- [5] Fischl B. FreeSurfer. Neuroimage 2012; 62: 774–81.